
US and World Medical Care
Misdiagnosis can happen in private or public health care. Doctors who place profits ahead of providing high quality medical services to their patients can be found practicing in private and public health care systems i. In a free market these doctors would soon find themselves out of business, but here in Saskatchewan doctors are paid by Medicare regardless of the quality of care provided.
Public health care demands that doctors help ration care to save the system money. Here in Saskatchewan the regional health authorities allocate money to diagnostic tests and surgeries. Is there a rubric to the rankings. If you look at patents on medicinal items, Israel is first, and American is 2nd. If there is a high percentage on low costs, but no reference to innovative discoveries, I also disagree.
This is choice in the US if you get cancer the chances you will go bankrupt. In the European countries all your treatment is paid for, prescriptions are often free for a number of years after diagnosis. In most European countries the life expectancy is higher than the US and we spend much less than the US. People need too look at the facts and move away from their suspicions of socialised. These comparisons are for the most part meaningless, yet we keep trudging them out as if there was some gem to be revealed.
All of the data comes from self-reporting entities. So why the disparity?
- Countries with the Best Health Care Systems.
- Dicker Hintern im Café auf Eis 2: Neue erotische Geschichten (German Edition)?
- Health care in the United States - Wikipedia.
- U.S. Health in International Perspective: Shorter Lives, Poorer Health.!
- Navigation menu.
- Primary Sidebar.
Naw that would harken to much back to the days of the USSR. The US usually ranks lower in these studies because there is less incentive to hide data-sets or pad stats on outcomes. Do we not see some correlation between the incentives provided by governments as part of reimbursement and the outcomes that get reported? Is there any disincentive in those very same countries for skewing self-reported data? I know people will want to believe what they want to believe, but to rely on these data sets as being meaningful for policy positions is to build your house out of a deck of cards.
Barnum is alive and well. A society of sheep that think they are individuals. Heather, if it were true that privitization spurs innovation, we would not rank 37th. The fragmentation and decentralization of healthcare administration and finance in the United States has created fiefdoms, largely for the benefit of administrators more than the actual people who provide care to patients.
We have crap healthcare in the U. No true… these are just political terms… the question and debate is deeper than politics. Right or wrong, good or bad, this is the french mentality. This debate in the US will only be resolved when we can answer this question. Free market capitalism favors healthcare as privilege and its in the blood of every American republican, democrat, etc.
Like it or not, this is who we are… This is how our society was built. The french see paying taxes to support their healthcare system as totally reasonable. Taxes are an anathema to almost every American. Government is an essential component of Democracy. Taxes are like dues to be a member of the democracy. Do I want my life run by huge corporations? No, I want a government that can control those corporations whose only duty is their executives and their largest shareholders.
Your outlook is strictly a Republican outlook. It may be shared by some Democrats, but not many. I grew up with an anesthisiologist at each and of the dinner table. I was for National Health Care then and I am for it now, even more so. My sister-in-law is a Harvard MS family doc who is extremely discourage with the devolution of US healthcare into the mess that it now is. Relatively few Canadians live in Seattle and very few Europeans. Healthcare is one of the reasons.
Free markets do not exist where pricing is not transparent. Healthcare is the most expensive thing in most Americans lives but nobody, including the doctors knows the price of any medical service. So if you wanted to compare prices from one place to the other, or given the extreme costs in the US, send out your procedure for bids.
Once again this is a system that has been completely taken over by huge corporations. Secondly when you restrict the number of physicians both internally and externally from outside the US it is absolutely NOT a free market. This has been going on since I was a kid in the 50s at least. There are many thing wrong with her story. Most basically, whereas she reveres competition as a trait of capitalism as most of its defenders do, every capitalist from day one strives and struggles to eliminate competition, and by eliminating competition they have brought us to a place of less choice due to 6 major Big Banks, 5 manufacturers of household appliances, a handful of major health insurance companies, and on and on.
And the profits that she praises and defends mean health insurance companies, to increase profits, are motivated to find innovative ways to pay out less in benefits while charging more for premiums. Dave, I think competition leads to more choice for consumers. The banking and health care insurance industries are both heavily regulated which ultimately impacts consumer choice. Thank goodness I still have options for banking and buying various household appliances. Heather, you and people like you are the problem. The GOP has you buffaloed with their scare tactics.
People are made to suffer to what end? And that seems to be a very good thing in this case. In America, we are made by the government to have insurance on our cars, our public schools are paid for by taxes, our public libraries, too. Time to recognize the new world, folks. Universal coverage just sounds better to those who are so paranoid about socialism. Fast forward to today August 3rd ……….. Medicare is socialized medicine. Medicaid is socialized medicine. Healthcare for vets is socialized medicine. I had far more problems, however, when I was dependent upon profit-motivated companies to provide me with health insurance.
We need to stop thinking in terms that create knee-jerk reactions and start thinking about what works best. Road construction and maintenance, railroad systems, law enforcement, fire protection and many.
World Health Organization’s Ranking of the World’s Health Systems | www.newyorkethnicfood.com
So is the U. But doctors, drugs companies, medical equipment manufacturers, continue to operate privately and for profit. The example lower down of a UK patient refused an operation in the US, was a patient expecting the UK to fund care from taxation. There are plenty of examples of US patients refused care by their insurer. And here we are with the lowest rated health care in the developed world while spending the largest percentage of our GDP.
List by the World Health Organization: France and Sweden 9 USA: Worried by the growth of the socialist movement, the Social Democratic Party in particular, Bismarck instituted the Anti-Socialist Laws in Socialist organizations and meetings were forbidden, as was the circulation of socialist literature.
In , Germany became a nation state. Bismarck worked closely with large industry and aimed to stimulate German economic growth by giving workers greater security: Universal can be socialized medicine or it can be non-socialized as in Canada. The doctors here have their own business and their pay is dependant on seeing patients unlike the UK method where they work for the government,. Canada has socialized medicine. Our universal health care system called Medicare is financed through taxation. It features compulsory government insurance and the government allocates funding and resources.
Doctors do not have the freedom to set their own prices for their professional services and patients do not have the freedom to spend their own money on medically necessary services. It boggles the mind that you can have such a narrow minded short sighted attitude towards basic social responsibility. You are obviously in excellent health greedily clutching your dollars close to your chest. The American system is madly expensive due to the insane attitude that everyone can make a buck by using a lawyer to rob the rest of society through questionable lawsuits.
This forces the doctors to take out gigantic malpractice insurance policies which cost them an absolute fortune. The Pharmaceutical companies charge maniacal prices for drugs that should be for the benefit of the patients, not the stockholders. Medical care is not rationally about making the biggest profit but that is apparently the American way.
In the 36 countries that have better care than America, there is still private healthcare and private insurance but there is basic care for all and those same private doctors are simply required to spend a portion of their time and business caring for the public sector not just the government workers and ex government people. Wait until you are denied treatment because your insurance is not good enough. Your arguments do not hold water. No mal-intent toward anyone is implied or literal. The Canadian and American systems are similar in that third-parties, not doctors and patients, make all the decisions regarding pricing, delivery, payment, and now the value of medical services.
This false economy is very lucrative for some. I think all patients, regardless of their material wealth, should have the freedom to spend their own money on their own health care. I can only hope it comes north! To expand government control over already government regulated areas seems insane.
Balance budget and reduce national debt before adding more responsibility and money to a incompetent government, regardless of party. You make a valid point. We are being scammed upside down and sideways in the U. Consider the cost per citizen right now in the U. The top five countries cost around half that. Medicare costs certainly suggests that healthcare in the hands of the U. If we can stop lining the pockets of private insurance companies, we can afford the taxes necessary to invest in a better quality of life.
The World Health Organization said that Columbia has one of the worst health care systems in the world yet, they ranked them 22 because they had equal access to that terrible system. Typical of liberal think. I think you misread that a bit. When you combine that with the fact that we are the most expensive and rank horribly in the accessibility categories, I think 37 is almost generous. The US health care system is so screwed up it makes it impossible for most people to retire because of the high cost of insurance—even the new Obama care is unaffordable.
Third world countries have better health care systems than us. I can only attribute it to the greed of the people who run this country. As said earlier, our government treats health care as a privilege for those who can afford it. That is the way health care should be! I am a healthcare practitioner and most of my constituients share the exact sediments …kudos. The WHO rankings are completely devoid of any common sense.
Ranking third world countries higher than the US is completely ridiculous. Use your brains people. Why in the world should it be the same across the board? There is a case going on right now where a nunnary is being charged tens of millions over that. Why should a single or not male be responsible for mammograms and other female care? I extremely disagree with the push for privitisation in my home country of Australia. Many years have gone past where I have had no need for the medical system.
Take care of the people around you, simple! In my opinion it has been cunningly exploited by privitisation advocates as justification to leave their brothers and sisters out in the cold. A business has a primary goal to make more money than it did the year before! The motivations behind systems of care, governance and infrastructure right across the board in most places need to be addressed. Everyone pays their percentage, one that is adequate for research too.
By that system the need for profit is taken out of the equation, reducing cost. Medical advancements made in reserched tech. With patients not needing insurance approval or lump sums of cash to get what they need to survive or have quality of life, the knock on effects to society and the way we think about caring for others is a step in the right direction we all need.
Many doctors are now opting out of socialized medicine in the USA and offering fee for service directly to their patients. Where do you live????? You are free to go to any doctor you want, as many times as you want. The quality is somewhat regulated — there are very few medical education systems in the world that Canada will accept doctors from without requiring further medical education.
Some are paid on a capitation basis — each patient in their roster worth so much per year — and if that patient sees another doctor, their family doctor may be charged for it incentive to keep their patients healthy! No one has more access to healthcare than anyone else in Canada. Everyone is free to choose to buy their healthcare elsewhere. You pay privately for plastic surgery, or fly to Thailand for breast implants, or the Philippines for faith healing or the States for whatever you want. So what if a country of people had all of the worlds best doctors and only people had access to them?..
The others would just die, or go bankrupt getting the proper care.. The capitalist approach certainly does stimulate research, but not necessarily for effective cures. Often times it creates marketing for ineffective cures, that the company holds patents on and has the means to promote.
Other times it creates ailments and syndromes to fit products it has on the shelf. The mere fact that Cuba,an impoverished nation, ranks very near to the US in effective healthcare, belies the capitalist argument. I think it breaks down to health care for profit. The motivation will always be to improve the bottom line. Genetics should make health care better yet for insurance companies they regard this as a new cash tool. Your genetics will help identify the possible probability of your future health care failure and you will be assessed on these risk also. I am a baby boomer and it was easy to believe it and it was for most things for a long time.
It is not what is required but simply what is politically feasible or possible. What can be done that will appease the electorate without negatively affecting our fund raising for the next election which is always two years away. Bad power and mostly greed are killing my southern friends and for the most part, all we can do is watch.
If I can make but one humble suggestion in planning the future for next generation: If you want to make America great again consider giving the same reverence to health care and education as you do the second amendment and gun control. And one more thing when TV news show the latest escapade of the Kardashians switch to the BBC and get a different take on major events and question what you hear. One version is never enough. Admin — This is not the source for the data you cite. There are a variety of tables in the WHO report which rank the countries on different criteria, thus moving the order around.
Andy, where do you get your info??? The WHO did not say Columbia has one of the worst!! In fact, they have one of the best. I know people from the US that go there specifically for their healthcare. You know little about this, based on your last comment you must be a conservative that falsely believes that the US has the best of everything. Oh yes it is….. Talk about all hell breaking loose. Then you will understand that the ACA has very little to do with health care. Of course everyone thinks they are as or more important than the next guy. We are a fast food society which expects everything now, regardless of how hungry you are.
As someone who has experienced both health care systems the US and Canada first hand I can tell you, the wait times are not much different. However, in the US if you have private insurance, you will be greeted with open arms like your checking into the Hyatt Regency. In Canada you are greeted with disdain and told to sit down. In the US the floors are shinny buffed with an expensive machine daily using some kind of toxic cleaner and wax. In Canada the floors are dull but clean having been cleaned with some environmentally safe cleaner but without the special polymer based coating.
Canadians are mostly treated like cattle. The quality of health care is not much different depending on your condition. The US has centers of excellence which do advanced research and are well funded. In Canada there is advanced research on a much smaller scale. This is all true — but only for the wealthy Americans. In Canada, at least everyone has a fair and equal chance to seek treatment. I have lived in both countries. Received and had relatives receive treatment in both countries.
You pay for treatment there, true. But we pay for it here, too. WE all know should know whats so moronic about your points. Lets follow your logic and give some examples 1. Because in America we have wide roads, so we all have must have great cars. Because there are more big house in America than most countries, then we all must have decent housing, 3. Since we have the most doctors, we all must have decent healthcare. We have the biggest buildings then we must all be doing great. Since we have more freedoms, then there must be less people breaking the laws and less people per capita in jail.
Since we have more people, we should have more tax revenue. We believe in god, so therefore we must be right. When Canadian politicians and bureaucrats leave the country to seek medical care they go to the United States. One has to be a very wealthy Canadian to seek care in the USA. Those who have no health insurance in the USA go to ER when they are often in dire situation and would never get a knee replacement if needed. No one in Canada goes without health care.. Everyone gets what they need though elective requires wait. The Affordable Care Act, if implemented, will produce an additional demand for services which the existing stable of primary care doctors will be unable to fill, particularly in economically depressed areas.
Training additional physicians would require some years. Lean manufacturing techniques such as value stream mapping can help identify and subsequently mitigate waste associated with costs of healthcare. In , coronary artery disease , lung cancer , stroke , chronic obstructive pulmonary diseases , and traffic accidents caused the most years of life lost in the US. Low back pain, depression , musculoskeletal disorders , neck pain, and anxiety caused the most years lost to disability. The most deleterious risk factors were poor diet, tobacco smoking, obesity, high blood pressure , high blood sugar , physical inactivity, and alcohol use.
Alzheimer's disease , drug abuse, kidney disease and cancer, and falls caused the most additional years of life lost over their age-adjusted per-capita rates. Between and , among the 34 countries in the OECD, the US dropped from 18th to 27th in age-standardized death rate. The US dropped from 23rd to 28th for age-standardized years of life lost. It dropped from 20th to 27th in life expectancy at birth. It dropped from 14th to 26th for healthy life expectancy. According to a study conducted at Harvard Medical School by co-founders of Physicians for a National Health Program , a pro-single payer lobbying group, and published by the American Journal of Public Health , lack of health coverage is associated with nearly 45, excess preventable deaths annually.
Goodman for not looking at cause of death or tracking insurance status changes over time, including the time of death. A study by former Clinton policy adviser Richard Kronick published in the journal Health Services Research found no increased mortality from being uninsured after certain risk factors were controlled for. A study of international health care spending levels published in the health policy journal Health Affairs in the year found that the United States spends substantially more on health care than any other country in the Organisation for Economic Co-operation and Development OECD , and that the use of health care services in the U.
The authors of the study conclude that the prices paid for health care services are much higher in the U. Uninsured Americans are less likely to have regular health care and use preventive services. They are more likely to delay seeking care, resulting in more medical crises, which are more expensive than ongoing treatment for such conditions as diabetes and high blood pressure. A study published in JAMA concluded that uninsured people were less likely than the insured to receive any medical care after an accidental injury or the onset of a new chronic condition.
The uninsured with an injury were also twice as likely as those with insurance to have received none of the recommended follow-up care, and a similar pattern held for those with a new chronic condition. In researchers with the American Cancer Society found that individuals who lacked private insurance including those covered by Medicaid were more likely to be diagnosed with late-stage cancer than those who had such insurance.
The treatment given to a patient can vary significantly depending on which health care providers they use. Research suggests that some cost-effective treatments are not used as often as they should be, while overutilization occurs with other health care services. Unnecessary treatments increase costs and can cause patients unnecessary anxiety.
The way the Health care system tries to eliminate this problem is through cost sharing tactics like co-pays and deductibles. If patients face more of the economic burden they will then only consume health care when they perceive it to be necessary. According to the RAND health insurance experiment, individuals with higher Coinsurance rates consumed less health care than those with lower rates. The experiment concluded that with less consumption of care there was generally no loss in societal welfare but, for the poorer and sicker groups of people there were definitely negative effects.
These patients were forced to forgo necessary preventative care measures in order to save money leading to late diagnosis of easily treated diseases and more expensive procedures later. With less preventative care, the patient is hurt financially with an increase in expensive visits to the ER.
The health care costs in the US will also rise with these procedures as well. More expensive procedures lead to greater costs. One study has found significant geographic variations in Medicare spending for patients in the last two years of life. These spending levels are associated with the amount of hospital capacity available in each area. Higher spending did not result in patients living longer. Primary care doctors are often the point of entry for most patients needing care, but in the fragmented health care system of the U.
For example, a Harris Interactive survey of California physicians found that:. According to an article in The New York Times , the relationship between doctors and patients is deteriorating. Doctors may focus on diagnosis and treatment, while patients may be more interested in wellness and being listened to by their doctors. Many primary care physicians no longer see their patients while they are in the hospital; instead, hospitalists are used. The health care system in the U. There are hundreds, if not thousands, of insurance companies in the U.
This system has considerable administrative overhead, far greater than in nationalized, single-payer systems, such as Canada's. There has been a shift in the type and distribution of administrative expenses over that period. The cost of adjudicating claims has fallen, while insurers are spending more on other administrative activities, such as medical management, nurse help lines, and negotiating discounted fees with health care providers. The largest increases in administrative costs were in customer service and information technology, and the largest decreases were in provider services and contracting and in general administration.
Variations in administrative costs between private plans are largely attributable to economies of scale. Coverage for large employers has the lowest administrative costs. The percentage of premium attributable to administration increases for smaller firms, and is highest for individually purchased coverage. Most Americans pay for medical services largely through insurance, and this can distort the incentives of consumers since the consumer pays only a portion of the ultimate cost directly.
Enrollment rules in private and governmental programs result in millions of Americans going without health care coverage, including children. Medicaid, which is available for those under certain income levels, does not guarantee access as physicians may elect to not accept Medicaid patients due to slow reimbursement, complex regulations, too much paperwork, and the necessity for extra staff to process the excess paperwork. The lack of coverage results in death due to lack of needed care [].
Mental illness affects one out of six adults in the United States. That is about A report by the U. The Paul Wellstone Mental Health and Addiction Equity Act of mandates that group health plans provide mental health and substance-related disorder benefits that are at least equivalent to benefits offered for medical and surgical procedures. The legislation renews and expands provisions of the Mental Health Parity Act of The law requires financial equity for annual and lifetime mental health benefits, and compels parity in treatment limits and expands all equity provisions to addiction services.
Insurance companies and third-party disability administrators most notably, Sedgwick CMS used loopholes and, though providing financial equity, they often worked around the law by applying unequal co-payments or setting limits on the number of days spent in inpatient or outpatient treatment facilities.
Prior to the Patient Protection and Affordable Care Act , medical underwriting was common, but after the law came into effect in it became effectively prohibited. Health disparities are well documented in the U. The average senior fills 38 prescriptions annually. There is considerable research into inequalities in health care. In some cases these inequalities are caused by income disparities that result in lack of health insurance and other barriers to receiving services.
In other cases, inequalities in health care reflect a systemic bias in the way medical procedures and treatments are prescribed for different ethnic groups. Raj Bhopal writes that the history of racism in science and medicine shows that people and institutions behave according to the ethos of their times.
The consistent and repeated findings were that black Americans received less health care than white Americans — particularly when the care involved expensive new technology. The Food and Drug Administration FDA [] is the primary institution tasked with the safety and effectiveness of human and veterinary drugs. It also is responsible for making sure drug information is accurately and informatively presented to the public.
The FDA reviews and approves products and establishes drug labeling , drug standards, and medical device manufacturing standards. It sets performance standards for radiation and ultrasonic equipment. One of the more contentious issues related to drug safety is immunity from prosecution. In , the FDA reversed a federal policy, arguing that FDA premarket approval overrides most claims for damages under state law for medical devices.
In this was confirmed by the Supreme Court in Riegel v. On June 30, , an FDA ruling went into effect extending protection from lawsuits to pharmaceutical manufacturers, even if it was found that they submitted fraudulent clinical trial data to the FDA in their quest for approval. This left consumers who experience serious health consequences from drug use with little recourse.
On March 4, , an important U. Supreme Court decision was handed down. Levine , the court asserted that state-level rights of action could not be pre-empted by federal immunity and could provide "appropriate relief for injured consumers. During the s, the price of prescription drugs became a major issue in American politics as the prices of many new drugs increased exponentially, and many citizens discovered that neither the government nor their insurer would cover the cost of such drugs.
Per capita, the U. Such governments should either deregulate their markets, or raise their domestic taxes in order to fairly compensate U. In turn, pharmaceutical companies would be able to continue to produce innovative pharmaceuticals while lowering prices for U.
Democrats have charged that the purpose of this provision is merely to allow the pharmaceutical industry to profiteer off of the Medicare program. Critics note that drug advertisements cost money which they believe have raised the overall price of drugs. When health care legislation was being written in , the drug companies were asked to support the legislation in return for not allowing importation of drugs from foreign countries. In , prior to the major healthcare reform in , Americans were divided in their views of the U. Much of the historical debate around healthcare reform centered around single-payer health care , and particularly pointing to the hidden costs of treating the uninsured [] while free-market advocates point to freedom of choice in purchasing health insurance [] [] [] and unintended consequences of government intervention, citing the Health Maintenance Organization Act of The costs of these provisions are offset by a variety of taxes, fees, and cost-saving measures, such as new Medicare taxes for high-income brackets , taxes on indoor tanning , cuts to the Medicare Advantage program in favor of traditional Medicare, and fees on medical devices and pharmaceutical companies; [] there is also a tax penalty for citizens who do not obtain health insurance unless they are exempt due to low income or other reasons.
The first open enrollment period of the Affordable Care Act began in October Prior to this period, access to healthcare and insurance coverage trends were worsening on a national level. A large, national survey of American adults found that after the act's first two enrollment periods, self-reported coverage, health, and access to care improved significantly. Furthermore, insurance coverage for low-income adults were significantly greater in states that expanded Medicaid in comparison with states that did not expand Medicaid. Those insured by Medicaid tend to report fair or poor health, as opposed to excellent or very good health.
In May , the state of Vermont became the first state to pass legislation establishing a single-payer health care system. The legislation, known as Act 48, establishes health care in the state as a "human right" and lays the responsibility on the state to provide a health care system which best meets the needs of the citizens of Vermont. After reviewing the costs and procedures for implementing such a program, the state decided against such a measure in late Inside the final version of the bill was a repeal of the individual mandate in the Affordable Care Act, which required individuals and companies to get healthcare for themselves and their employees.
It was this mandate which kept healthcare costs down under the PPACA by promoting cost sharing over a larger pool. Although the Affordable Care Act and the American Health Care Act both propose tax cuts in order to make insurance more affordable for Americans; however, each of these bills affected Americans in different ways.
World Health Organization’s Ranking of the World’s Health Systems
Young people because individuals between the age of 20 and 30 will see drops in the premiums they pay within their plans. In addition, those in urban areas can also benefit from the plan because under Obamacare tax credits were designated also by the cost of local healthcare, but the American Health Care Act does not take this into consideration although rural healthcare is generally more expensive due to the lack of hospitals and available services.
Among those immigrants who became citizens, In each age and income group, immigrants are less likely to have health insurance. Undocumented immigrants within the United States do not have access to government funded health insurance. Although The Affordable Care Act allows immigrants to receive insurance at a discounted rate, the same does not go for those without US citizenship.
From Wikipedia, the free encyclopedia. This article needs to be updated. Please update this article to reflect recent events or newly available information. Obama administration proposals Public opinion Reform advocacy groups Rationing Insurance coverage. Free market Health insurance exchange Nationalized insurance Publicly-funded Single-payer Canadian vs. All-payer rate setting Capitation Fee-for-service Global payment. This section is empty. You can help by adding to it. List of causes of death by rate. Medical centers in the United States.
Physician in the United States. This section is written like a personal reflection, personal essay, or argumentative essay that states a Wikipedia editor's personal feelings or presents an original argument about a topic. Please help improve it by rewriting it in an encyclopedic style.
Ranking the Top Healthcare Systems by Country
April Learn how and when to remove this template message. Hospital Quality Incentive Demonstration. Comparison of the healthcare systems in Canada and the United States. Years of potential life lost. Health insurance coverage in the United States. Race and health in the United States. Regulation of therapeutic goods in the United States. This article appears to contradict the article Prescription drug prices in the United States. Please see discussion on the linked talk page.
October Learn how and when to remove this template message. Prescription drug prices in the United States. Health care reform in the United States. Immigrant health care in the United States. Retrieved December 22, Retrieved December 1, American Journal of Public Health. Retrieved July 12, Retrieved May 26, Life Expectancy at Birth". Retrieved April 22, Journal of the American Medical Association. Retrieved July 11, Explicit use of et al. Health in International Perspective: Woolf and Laudan Aron, Eds.
The National Academies Press. Treatment goals for controlling hypertension, elevated serum lipids, and diabetes rely heavily on the use of prescription drugs, and the United States has higher per capita consumption of pharmaceuticals than peer countries Morgan and Kennedy, ; Squires, Evidence is available on how the United States compares with other countries in achieving specific cardiovascular and diabetes treatment targets.
The use of preventive drugs for people at risk of cardiovascular disease is more common in the United States than in Europe Crimmins et al. In a comparison of medication use in the United States with 10 European countries, Thorpe and colleagues found that use of antihypertensive agents did not differ significantly but that use of cholesterol-lowering drugs and medication for heart disease was greater in the United States than in Europe. A National Research Council study also documented that patients with high blood cholesterol and hypertension were more likely to receive medications in the United States than in comparable countries.
A analysis of survey data collected in the s demonstrated that blood pressure was more effectively controlled in the United States than in Canada or Europe Wolf-Maier et al. There is also some evidence that the speed of cardiovascular care for acute coronary syndrome in the United States may match or exceed that of Europe Goldberg et al. Diabetes Care The United States may be less exemplary than other countries in meeting testing and treatment targets for diabetes care. In one survey, patients with diabetes in half the countries were more likely to report a recent hemoglobin A1c test, foot examination, eye examination, and serum cholesterol measurement than patients in the United States Schoen et al.
Case-Fatality Rates A measure of the quality of care of life-threatening illnesses is the probability of death following treatment, also known as the case-fatality rate. An earlier OECD analysis, based on mortality data from the s, reported that the United States had low case-fatality rates at 30 days, 90 days, and 1 year after acute myocardial infarction Moise et al.
In a comparison of 5-year mortality rates following acute myocardial infarction among U. In-hospital case-fatality rates for acute myocardial infarction in 16 peer countries. Data are for or nearest year; data apply to deaths within 30 days of admission for acute myocardial infarction. One study calculated the ratio between diabetes mortality for — and incidence at ages 0—39 in 29 industrialized countries.
The United States had the 10th highest ratio—higher than all Western European countries, Canada, Australia, and New Zealand—but the comparison was subject to a variety of limitations Nolte et al. Other Clinical Outcomes Apart from time-limited case-fatality rates, the panel found no comparable data for comparing the effectiveness of medical care across countries. Data are available for comparing cancer survival rates, which are generally higher in the United States, but cancer survival is confounded by lead-time and length biases introduced by screening Ciccolallo et al.
This screening artifact could explain both the higher incidence Thorpe et al. In one survey, U. Another study reported that day readmission rates for a common form of myocardial infarction were higher in the United States than in Canada, Australia, New Zealand, and 13 European countries Kociol et al. Little evidence exists to compare the frequency of hospitalization for ambulatory care-sensitive conditions Institute of Medicine, d —a proxy for the quality of outpatient care—except for two conditions asthma and diabetes , and they portray different patterns.
Although OECD b data for peer countries indicate that the United States has the highest asthma hospitalization rate among persons age 15 and older, the U. Hospital admissions for asthma in 16 peer countries. Rates are age-standardized and based on data for or nearest year. Hospital admissions for uncontrolled diabetes in 14 peer countries. Rates are age-sex standardized, and they are based on data for or nearest year.
Outcomes after organ transplantation offer an interesting comparative picture of the quality of perioperative care and subsequent chronic care in the United States. Dawwas and colleagues compared outcomes for adults who underwent a first single organ liver transplant between and in the United Kingdom or Ireland with those in the United States. Risk-adjusted mortality in both countries was generally higher than in the United States during the first 90 days, equivalent between 90 days and 1 year post-transplantation, and lower than the United States after the first post-transplant year.
Another imperfect measure of the performance of health care systems is to estimate the mortality that is considered amenable to health care Nolte and McKee, ; Rutstein et al. Relying on the assumption that all deaths from a list of more than 30 causes and 50 percent of deaths from ischemic heart disease could be averted by better health care, 15 Nolte and McKee concluded that the United States had the highest amenable mortality rate among 16 countries Nolte and McKee, Building on this analysis for a larger set of countries, the Commonwealth Fund Commission on a High Performance System concluded , p.
Up to , fewer people would die prematurely if the U. Clinically recorded errors are also imperfect and are only available across countries for a few indicators. A factor that could diminish the effectiveness of health care in the United States is disruptions in the care delivery process.
For many years, quality improvement programs and health services research have recognized that the fragmented nature of the U. Differences in medical error rates between countries have an independent association with breakdowns in care coordination Lu and Roughead, The only detailed data to compare care delivery practices across countries come from surveys conducted each year by the Commonwealth Fund. These data have a variety of limitations.
For example, they rely on perceptions of patients and physicians rather than independently documented outcomes. Although the surveys have been administered annually since to thousands of patients and physicians in up to 11 countries, they include dozens of questions about care delivery practices that have varied in wording and administration methods over the years. However, a consistent pattern emerges in the U. Survey Findings from Commonwealth Fund Surveys.
Attention to clinical detail Practice knows important information about medical history. Among surveyed countries, U. Could these coordination problems reflect the large proportion of U. In , the Commonwealth Fund stratified the survey responses of chronically ill patients based on their insurance status. As shown in Figure , coordination problems were more common among the uninsured, as would be expected, but large proportions of insured patients up to 43 percent also reported difficulties getting appointments, inefficient care or wasted time, and medical test or record coordination problems.
One in four insured patients was sufficiently dissatisfied to recommend rebuilding the health system Schoen et al. Frequency of complaints among insured and uninsured U. Based on surveys of patients with chronic illnesses conducted by the Commonwealth Fund. Adapted from Schoen et al. The evidence reviewed above supports the following conclusions: More data are available for comparing health care systems across countries.
American patients and primary care physicians are more dissatisfied with their health care system and are more likely to want major reforms than are patients and physicians in other countries. A conspicuous problem in the United States is the lack of universal health insurance, something recent reforms have sought to address, but deficiencies in access and quality are pervasive and plague even insured and high-income patients.
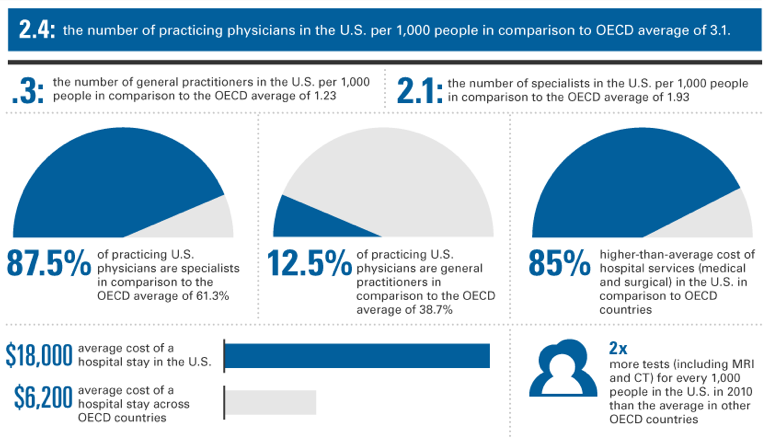
The United States has fewer practicing physicians per capita than comparable countries. Specialty care is relatively strong and waiting times for elective procedures are relatively short, but Americans have less access to primary care. Continuity of care is weaker in the United States than in other countries: Compared to people living in comparable countries, Americans do better than average in being able to see a physician within 1—2 days of a request, but they find it more difficult to obtain medical advice after business hours or to get calls returned promptly by their regular physicians.
There appear to be differences in the quality of hospital and ambulatory care across countries. Compared with most peer countries, U. However, quality appears to drop off in the transition to long-term outpatient care. Pharmacotherapy and control of blood pressure and serum lipids are above the average for comparable countries. However, systems to manage illnesses with ongoing, complex care needs appear to be weaker. Long-term care for older adults is less common.
Confusion, poor coordination, and miscommunication are reported more often in the United States than in comparable countries. Moreover, these problems are reported in large numbers by insured and above-average income patients. Whether poor coordination of complex care needs for chronic conditions—such as asthma, congestive heart failure, depression, and diabetes—is contributing to the U. The current evidence is mixed.
- The Crisis of the 17th Century: Religion, the Reformation and Social Change (Religion, the Reformation, and Social Change).
- Dylan’s Time-Flying Adventures with the Holy Spirit: David and Goliath?
- Health care in the United States.
Testing of patients with diabetes may be less common in the United States than in some other countries, but only five peer countries have a lower rate of hospitalizations for uncontrolled diabetes. The quality problems with U. The same surveys that describe coordination problems also suggest that U. Problems with health care in the United States are important, but at best, they can explain only part of the U.
DEFINING SYSTEMS OF CARE
First, some causes of death and morbidity discussed in Part I are only marginally influenced by health care. For example, homicide and suicide together account for 23 percent of the extra years of life lost among U. Deficiencies in ambulatory care in the United States bear little on the large number of deaths from transportation-related injuries.
Access to emergency medical services and skilled surgical facilities could play a role, but there is no evidence that rescue services or trauma care in the United States are inferior to the care available in other countries see Box Other factors, ranging from road safety to drunk driving and socioeconomic conditions, may matter more Transportation Research Board, Second, although poor medical care could be plausibly linked to communicable and noncommunicable diseases, which claim 20—30 percent of the extra years of life lost in the United States see Chapter 1 , the available evidence for two common noncommunicable diseases—myocardial infarction and ischemic stroke—suggests that U.
The United States excels in performing screening tests that are known to reduce mortality. However, it is possible that the health disadvantage arises from shortcomings in care outcomes that are not currently measured and from gaps in insurance, access, and coordination. Even the measures that are available for myocardial infarction and stroke are limited to short follow-up periods after the acute event, and outcomes may deteriorate thereafter. Part I lists nine domains in which the U. Deficiencies in public health systems or in access to quality health care could conceivably play a role in each of these domains.
For example, the United States has a high rate of preterm births see Chapter 2 , a large proportion of which appear to be initiated by health care providers Blencowe et al. Higher death rates from HIV infection could relate to deficiencies in care. Third, even conditions that are treatable by health care have many origins, and causal factors outside the clinic may matter as much as the benefits or limitations of medical care. For example, smoking and obesity are heavily influenced by the environment and policy decisions see Chapters 5 and 7. Physicians play an important, but marginal, role in screening for unhealthy behaviors, measuring body weight, prescribing adjunctive pharmacotherapy to support smoking cessation or weight management, performing bariatric surgery for morbid obesity, and referring patients to telephone quit lines and other intensive behavioral counseling programs Fielding and Teutsch, ; Ogden et al.
Physicians can write prescriptions for antihypertensive drugs, statins, oral contraceptives, and antibiotics and antiretroviral agents for sexually transmitted infections and HIV infection. They can encourage healthy behaviors, but other factors exert greater influences on diet, physical activity, sexual habits, alcohol and other drug use, and needle exchange practices Woolf et al.
Pediatricians can remind parents to secure their children in car seats, but they cannot control motor vehicle crashes. Physicians can screen for and treat depression and be alert for suicidal ideation and signs of family violence but they have limited influence on the prevalence of firearms or the societal conditions that precipitate crime and violence. One difficulty in attributing the U. In some countries, patients are more likely to report problems. For example, Sweden consistently ranks among the healthiest countries in the OECD, but, in the Commonwealth Fund surveys, its patients were more likely than U.
Sweden has high hospitalization rates for uncontrolled diabetes Figure In , Switzerland had the highest male life expectancy among the 17 peer countries see Table , in Chapter 1 , but the availability of general practitioners is the second lowest see Figure Australia has the second highest male life expectancy of the peer countries see Table , in Chapter 1 , but it has the fifth highest case-fatality rate for ischemic stroke OECD, b. The Netherlands, which ranks highly on many surveys by the Commonwealth Fund, has historically had shorter life expectancy than some other comparable countries.
Various potential explanations could account for these inconsistencies.