
Muscle Testing for Weight Training Shoulder Injuries (SWIS Education Series - Vol. 54)
Return to Book Page. Optimal Muscle Training by Ken Kinakin. Ken Kinakin is a chiropractor, certified strength and conditioning specialist, and certified personal trainer. He also has competed in bodybuilding and powerlifting for more than 20 years. He regularly lectures in Canada and the United States to doctors and personal trainers on weight training, rehabilitation, and nutrition. He is on the Canadian and International Powerlif Ken Kinakin is a chiropractor, certified strength and conditioning specialist, and certified personal trainer.
Hardcover , Book with DVD , pages. To see what your friends thought of this book, please sign up. To ask other readers questions about Optimal Muscle Training , please sign up. Be the first to ask a question about Optimal Muscle Training. Lists with This Book.
Books by David Leaf (Author of KISS)
This book is not yet featured on Listopia. Curtis Cherry rated it really liked it Dec 23, Carson Patterson rated it really liked it Jun 20, Sean Austin rated it it was amazing Jan 11, Eric rated it liked it Nov 07, Trevor Pardy rated it liked it May 04, Ralph rated it really liked it Apr 07, Lynda rated it liked it Jan 25, This would still be within the 3-month time frame supported by Weinstein et al. The patient limited his lifting and physical activity for 3 weeks.
After 3 weeks, he could complete all of his own shopping and housework and resumed running 4. He also began lifting weights on his own in an attempt to strengthen his shoulder and improve his ability to push open doors or complete a push-up. Eleven weeks after the initial injury, the patient was experiencing no pain, and he could perform activities of daily living and lift heavy objects from the floor and overhead with minimal difficulty.
Despite a palpable click underneath the left scapula with overhead motions and horizontal adduction of the shoulder, the patient was able to run at his preinjury level and play golf. The result was an unstable scapula instead of a stable foundation required for movement by the articulation between the acromion and the clavicle. This functional deficit remained despite activity-specific attempts to strengthen that motion with scapular stabilization and chest-press weight training over a period of 2 months and was unlikely to change without surgical fixation.
Similarly, no change in the step deformity was apparent upon visual inspection. Eleven weeks after injury, the patient was seen for a preoperative examination to assess his baseline ROM and strength. Range of motion as reported in Table 1 was performed as described by Norkin and White 24 The exceptions to this were the combined movements of overhead reach and behind-the-back reach as described by Magee.
Several reports 27 — 29 have shown that goniometric measurements of shoulder ROM are reliable, especially when the measurements are taken by a single experienced clinician. In addition, manual muscle test scores for the internal and external rotators and middle trapezius muscle are known to have good intratester reliability. As a result, we believe that the ROM and strength measurements used in this case report were reliable. Beaton et al 34 reported a change of 5 to be the standard error of measurement for the DASH and thus the threshold for a minimal clinical difference.
On the general DASH form, the patient scored 9. Measurements for strength and ROM are described in Table 1. We did not assess the reliability of our own measurements. As a result of the functional deficit that remained after 12 weeks of conservative treatment, the patient consented to undergo a modified Weaver-Dunn CA ligament transfer to surgically reconstruct his AC joint. A modified Weaver-Dunn CA ligament transfer was completed as previously described. Upon completion of the surgery, the clavicle was stable in the anteroposterior direction with gentle manual manipulation.
No evidence of abutment between the clavicle and acromion was present with horizontal adduction or rotation. Following surgery, the patient was required to use a canvas shoulder sling with an immobilizing swath on a full-time basis for 6 weeks and was restricted from all lifting other than manipulating small objects such as utensils in his hand.
Optimal Muscle Training
After 3 weeks, follow-up radiographic images indicated that the space between the clavicle and acromion was in its surgically fixed position of approximately 3 mm. Strengthening was permitted for the wrist flexors and extensors, and the patient was encouraged to passively flex and extend his elbow with the arm supported on a table or countertop. Ten repetitions of passive range of motion PROM were completed independently for 2 to 3 sessions per day.
To maintain cardiovascular fitness, the patient rode a stationary bicycle sitting upright without use of the handlebars. Physical therapy began after 6 weeks of shoulder immobilization and a second postsurgical follow-up visit with the surgeon. In a supine position, the weight of the scapula would be supported by the treatment table and would not pull on the surgical graft as would happen in gravity-dependent positions such as sitting or standing.
The patient was allowed to complete isometrics for the shoulder and elbow and was encouraged to reach full glenohumeral PROM in external rotation. After a prolonged period of immobilization, a review of the musculoskeletal, cardiopulmonary, neuromuscular, and integumentary systems was performed. The patient was found to have restrictions in glenohumeral and elbow ROM, poor active scapular control, and atrophy of the left deltoid and upper arm musculature. He also had restriction and decreased mobility near the surgical incision due to the adherence of the skin to the underlying tissue.
Range of motion and manual muscle test results for the shoulder and elbow are listed in Table 1. Left shoulder flexion, abduction, and external rotation and elbow extension AAROM were decreased compared with the preoperative examination. Although the measured ROM for left glenohumeral internal rotation was higher than during the preoperative examination, the ROM was still less than the documented norms for that motion.
However, he did demonstrate restricted external rotation and internal rotation that are commonly associated with anterior and posterior glenohumeral capsular restrictions. The DASH questionnaire was again completed, and the scores were As expected, both of these scores changed more than the 5 to 15 points, which is reported to indicate clinically significant changes in upper-extremity function. Restricted ROM, loss of strength, and impaired motor performance are common after surgical reconstructions of the AC joint. A short-term goal of increasing left shoulder AAROM to 90 degrees of external rotation, degrees of flexion, and degrees of abduction was established to be achieved in 2 weeks.
Upcoming Events
Long-term, the patient wanted to resume his previous level of sports, including golf, bicycling, running, and recreational softball. In addition, he felt that completing 10 push-ups without difficulty would indicate a satisfactory resolution of his principal presurgical complaint of scapular instability with push-ups and opening heavy doors. Moreover, it would confirm a resolution of the mechanical instability corrected by the surgery. Initial treatment consisted of moist heat for 15 minutes and available AAROM with a straight cane guided by the uninvolved upper extremity or physical therapist assistance into shoulder flexion, abduction, and external rotation patient positioned supine.
At his second treatment session, continuous ultrasound over the anteroinferior glenohumeral joint capsule 2. Active range of motion and manual resistance were applied to the scapula in superior, medial, lateral, and inferior directions scapular clock , and ice was applied to the left shoulder for 15 minutes following treatment.
The patient was seen in the physical therapy clinic 3 times per week and assigned a daily home exercise program that emphasized isometric shoulder strength and glenohumeral and scapular ROM within the postsurgical restrictions Tab. A daily log of home exercises was maintained throughout the duration of physical therapy intervention. Because a gross restriction in posterior glenohumeral accessory motion was noted during the initial physical therapist examination, the physical therapist hypothesized that these symptoms may be secondary to a restricted posterior glenohumeral joint capsule or the early stages of an internal impingement of the supraspinatus muscle by the posterior glenoid rim.
The first method was performed by the physical therapist with the patient in a supine position and the shoulder in the open packed position. The second method was completed by the patient in a left side-lying position with his shoulder in 70 degrees of flexion. In both cases, the physical therapist or the patient passively moved the shoulder into internal rotation to the point of gentle stretch held 30 seconds for 5 repetitions. In addition, the grade III posterior glenohumeral joint mobilizations initiated during the second treatment session were emphasized by increasing the number of bouts to 7.
Elbow ROM activities continued, and the patient had no complaints of pain or loss of function other than transient stiffness attributed to the 6 weeks of immobilization. However, left scapular winging and anterior tipping were noted during open-chain motions such as shoulder elevation and prone horizontal abduction and flexion. This finding suggested that the inferior migration of the coracoid process and anterior tilt of the scapula were likely caused by either slight muscular tightness or weakness of the lower trapezius muscle. However, when the serratus anterior muscle was tested in the preferred, sitting open-chain position without support of the scapula by the treatment table, the muscle was not able to maintain the position of the scapula on the thorax when challenged with resistance by the examiner.
In addition to tightness in the muscles attaching to the coracoid process or weakness of the serratus anterior and lower and middle trapezius muscles, impaired neuromuscular control of these muscles following 6 weeks of immobilization and 4 additional weeks of limited shoulder movement also may have played a role in the winging and anterior tilt of the scapula.
- Hand-Me-Down Jack?
- Illumination: Spiritual Emergence and the Evolution of the Soul.
- Black Market.
- Introduction.
- Optimal Muscle Training by Ken Kinakin?
In order to strengthen the scapular stabilizing muscles, closed-chain exercises and assisted exercises for the lower trapezius and serratus anterior muscles were initiated. The patient also worked on strengthening at home by placing his arm at about degrees of abduction with the shoulder externally rotated and contracting the lower trapezius muscle to facilitate scapula depression and prevent anterior tilting.
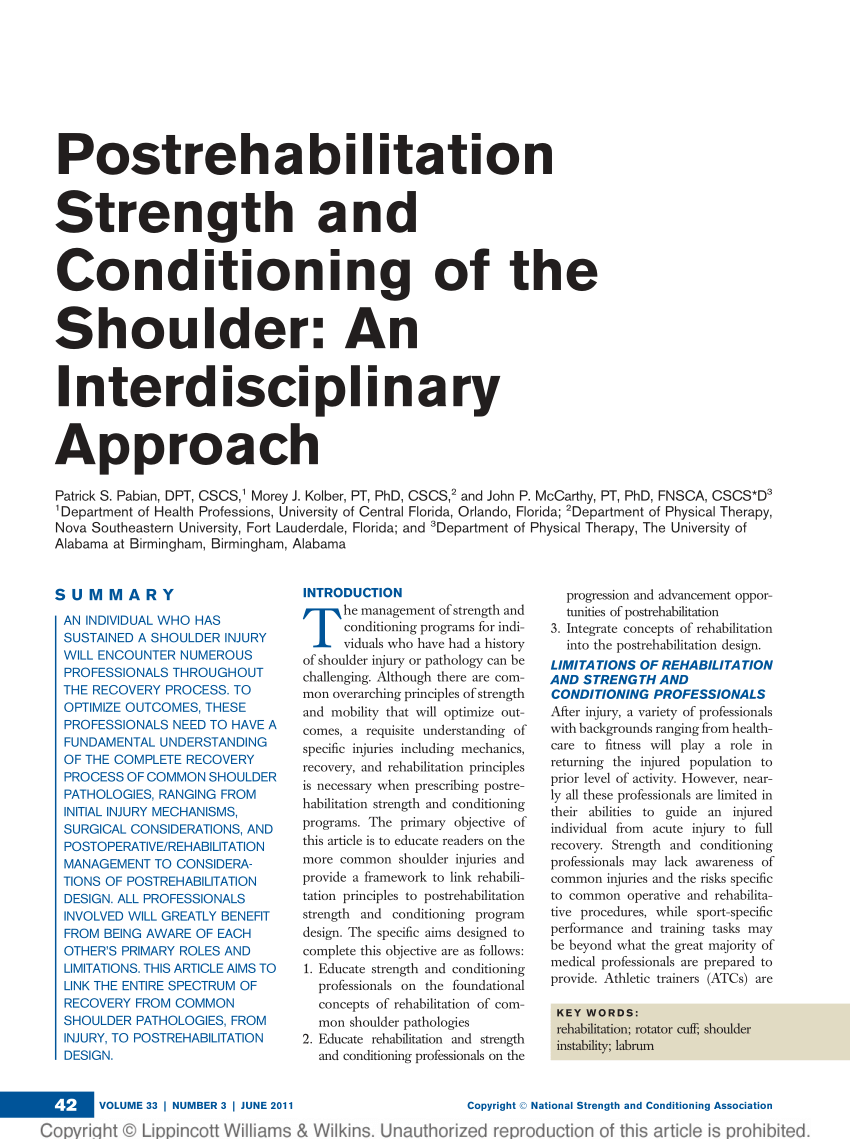
Push-up plus activity to strengthen the serratus anterior muscle: Shoulder extension in standing using minimal resistance from the Pro-Fitter Trainer: A starting position and B ending position. Partial weight bearing through the left upper extremity onto a Swiss ball: A in a bent-over position and B with the ball on the wall.
- Hand-Me-Down Jack!
- Books by David Leaf?
- Sophies Tutor!
- THREE TIMES A LADY: A Serial Killer Thriller.
- Case Description.
- .
- David Leaf (Author of KISS).
To address the deficit in glenohumeral ROM, joint mobilizations were continued with passive stretching. Glenohumeral joint distraction and mobilizations of the humeral head in the posterior, inferior, and anterior directions were performed with the humerus in the open packed position with neutral rotation or toward the end-range of external rotation. With the patient in this position, Maitland grade III oscillations were performed for 30 seconds, 5 repetitions in each direction, to facilitate humeral accessory motion.
Participants were asked to demonstrate performance of those activities that provoked shoulder pain. The intervention physical therapist assessed their task performance observationally and emphasized those specific recommendations eAppendix 2 for the related activities. The attention control intervention was designed as a sham intervention to give participants time and attention from a clinician. Participants randomly assigned to this group viewed a 1-hour instructional video emphasizing shoulder anatomy, mechanisms of injury, and general concepts in managing shoulder pain.
A handout on the video and an educational brochure regarding general shoulder care were provided to all attention control group participants. The information was intentionally general and did not contain recommendations to change behavior.
Outcome measures for each participant were assessed by the same physical therapist at baseline, at the end of the week intervention, and again at 4 weeks after the end of the intervention. Secondary outcome measures within the ICF domain of body function and structures included a single-item VAS 0—10 cm for rating shoulder pain 45 and measures of shoulder strength.
Measurement of shoulder muscle force production using an HHD has been shown to be highly reliable in people with SCI, with intraclass correlation coefficients for intrarater reliability from. It covers leisure-time activities, household activities, and work-related demands. Participants are asked to make an overall rating of their current life, taking everything into account.
It has shown both good validity and reliability and has been shown to correlate negatively with measures of depression and positively with measures of life satisfaction. To compensate for expected attrition, we planned to enroll 40 participants per group. Statistical analyses were conducted at the. Because our primary purpose was to establish the effects and functional impact of our intervention, we elected to complete the primary analyses on the evaluable participants ie, those participants who completed the intervention and returned for the immediate postintervention assessment.
Repeated-measures ANOVA models were used to determine the interaction effects of intervention group and time baseline versus immediate postintervention. When a significant interaction between group and time was identified, post hoc comparisons were conducted to determine whether the changes over time were significant within each intervention group.
In the latter case, each outcome variable was compared over time between the immediate postintervention assessment and the final assessment 4 weeks later. We also report the results of an intention-to-treat ITT analysis of all randomized participants across the 3 assessment times using a mixed linear model analysis to accommodate missing values. The means at each time interval using the ITT analysis include values from all participants regardless of whether they completed the invervention or subsequent outcome assessments.
Intervention group and time were included in the model as fixed effects, and the intercept of the dependent variable at baseline across participants was the random effect. Figure 3 shows the consort flow diagram. Among the individuals screened for eligibility, a total of 80 participants 40 per intervention arm were eligible for randomization and gave written informed consent.
Table 1 summarizes the demographic and clinical characteristics for the 80 randomized participants, stratified by intervention assignment. The remaining 7 participants were lost to follow-up. Reasons for withdrawal in the attention control group were: Six additional participants in the attention control group withdrew from the study after completing the immediate postintervention assessment but prior to the 4-week follow-up assessment. Five of the 6 participants were lost to follow-up, and 1 individual died from aortic dissection.
No significant differences in demographics or baseline outcome measures existed between participants who withdrew and those who completed the immediate postintervention evaluation. Adverse events AEs were monitored and reported according to the protocol approved by the Data Monitoring and Safety Committee. There were 27 cumulative AEs that occurred in 23 participants. The remaining 25 AEs were not related to the study, and 9 were considered serious. The exercise program was interrupted temporarily for 2 participants who had serious non—study-related AEs.
See a Problem?
Serious, non—study-related AEs associated with the attention control group were: Non—study-related, nonserious AEs in the attention control group were: Two of 4 participants who required additional instruction in exercise performance demonstrated an increase in resistance for the 8- and repetition maximum levels in all 4 exercises, indicating at least partial adherence. One participant increased resistance in only 1 of 4 exercises, and the other person did not increase the resistance in any of the exercises, indicating likely nonadherence to the exercise program.
Transfers were modified in 12 participants, with specific recommendations to avoid internal rotation of the shoulder, to keep hands on transfer surfaces, to lead with the painful arm, to lean the trunk forward, and to use a stool for an intermediate surface when the target transfer surface was significantly higher or lower than the wheelchair. Wheelchair propulsion technique or setup was modified in 6 participants, with specific recommendations to move the rear wheel axle forward, to avoid inclines, and to consider a lightweight wheelchair.
Data are reported as mean and standard deviation. Data are mean SD unless otherwise indicated. Pain levels on the WUSPI were similar, however, at the immediate postintervention assessment, regardless of whether specific movement optimization instruction was received Physical activity PASIPD scores and wheelchair propulsion speed were not significantly changed after the intervention in either group Tab. Although the average SII scores increased 8.
Data are mean scores SD unless otherwise indicated. P values for between-group comparisons were obtained from the interaction of treatment group and time using a repeated-measures analysis of variance. For participants in the attention control group, the high levels of shoulder pain recorded at the immediate postintervention assessment were not significantly reduced at the 4-week follow-up assessment Tab. Community activity levels, overall SQRL scores, and SF scores also were unchanged in both groups from the immediate postintervention assessment to the 4-week follow-up evaluation Tab.
This intervention was documented only anecdotally because it was not a formal part of the STOMPS trial, and no follow-up assessment was planned. Results of the ITT analysis of all 80 randomized participants across the 3 assessments were similar to those of the primary analysis, which included only participants who completed the intervention. There were no significant differences between groups in response to the intervention using the ITT analysis for the external rotation torque, wheelchair propulsion speed, the SII, the SF mental component score, and the remaining SF subscales.
P values for between—group comparison were obtained from the interaction of treatment group and time using a repeated—measures analysis of variance. We demonstrated a marked reduction in shoulder pain levels in individuals with SCI using a relatively simple home exercise intervention coupled with assessment and modification of performance technique for several UE weight-bearing activities. Consequently, this study provides the only evidence from a randomized controlled trial for the effectiveness of an intervention that includes exercise in reducing chronic shoulder pain in individuals with SCI.
The magnitude of the pain reduction is particularly noteworthy, given that the participants' average duration of shoulder pain was greater than 5 years Moreover, the extent of pain reduction demonstrated in this study is more than 2 times greater than the estimate of a minimal clinically important reduction of chronic pain in patients treated for rotator cuff disease 1.
This finding is contrary to our hypothesis and what would be expected, given the findings of Gutierrez and colleagues, 14 who documented a significant correlation between shoulder pain levels and both physical activity and community activity scores. However, the improvement seen in health-related QOL, particularly in scores on the role—physical and social functioning subscales of the SF, suggests that the reduction in shoulder pain allowed individuals to more successfully complete their social and life role activities.
This discrepancy in results might reflect differences between outcome measures in the quantification of activity. Both the PASIPD and the SII measure the frequency of performing specific activities prespecified by the test designer , whereas the SF permits the respondent to assess social activities and life roles in general to reflect those that are pertinent. The results of our randomized controlled trial generally are consistent with the few studies in the literature that investigated the impact of an exercise program on shoulder pain in individuals with SCI.
Our goal was to develop an exercise program that was effective, required minimal equipment, and was brief enough to minimize the added burden on participants who already have heavy self-care demands. The rotator cuff muscles were the primary focus of our strengthening protocol in this trial, which was most similar to that used in the study by Curtis and colleagues. The strengthening exercises used by Nawoczenski and colleagues 24 focused primarily on scapular muscles using electromyographic-guided exercise prescription, but also included an exercise for the shoulder external rotator muscles.